
Picture this: it's 6:47 AM on a Monday. A doctor and a Global Supply Lead managing a Phase III oncology trial opens her inbox. Twenty-three unread messages. One stops everything.
"Patients are here for their Week 16 infusion. We have no drug. What do we do?"
847 patients. 31 sites. 9 countries. A temperature-sensitive biologic with a four-month shelf life.
Here is what that Monday morning ultimately cost:
- $2.6 million in total direct costs
- $480,000 in IMP write-off; 180 units expired, gone
- 11 weeks of trial delay, pushing the database lock to Q1
- 1 protocol deviation filed with the regulator
- 0 of those outcomes were inevitable
68% of clinical trial delays are traced to supply chain risk identified too late. The average cost of a single day delay in a Phase III trial is $1.3 million. And the average gap between when a supply risk first becomes detectable and when it is detected is SIX weeks.
Six weeks during which the data was generating signals, and no one was reading them together.
In my work helping enterprise pharma organizations build decision-centric supply chains, I've come to think of this exact scenario as an architectural problem. The systems we use to run clinical trials aren’t connected to each other, and the organizational processes built on top of them aren’t designed to catch the signals that live hidden in those systems.
That's the root cause. Everything else flows from there.
Three Structural Failures in Clinical Trials Supply Chain Management
I want to be specific about this, because the "we need better visibility" conversation in clinical supply chains has been happening for a long time without solving the underlying problem. Dashboards aren't the answer if the data underneath them is still siloed and backward-looking.
There are three structural failures that create the detection gap. They compound each other, and you need to address all three.
Siloed Systems
A typical Phase III trial generates supply chain data across at least five distinct system categories: IRT for patient randomization and dispensing, SAP for materials planning and manufacturing orders, WMS at depots and CMO sites, CTMS for protocol and enrollment data, and CMO portals for external manufacturing status.
Each of those systems is authoritative for its own domain. None of them were designed to reveal the relationship between their data and the data in the system next to it.
Blind spots multiply at every handoff. The more hand-offs, the more blind spots.
Reactive Monitoring Built on Scheduled Reviews
This is the one I push hardest on when I'm working with supply chain leaders, because it's the assumption that's hardest to challenge: the idea that weekly batch release calls, monthly supply planning reviews, and bi-weekly inventory reports constitute "monitoring."
They don't. They constitute retrospective reporting.
A weekly inventory report tells you what happened last week. A monthly planning review tells you what your plan assumed three weeks ago. By the time an anomaly surfaces in a scheduled review, it has already been an anomaly for days or weeks.
The teams running these reviews aren't failing. The monitoring architecture is. It was designed for a world where data was slow and scarce. We now live in a world where data is fast and abundant, and the monitoring architecture hasn't caught up.
No Predictive Layer for Early Signal Detection
Even organizations that have invested seriously in dashboards and real-time data feeds, frequently lack the analytical layer required to turn data streams into forward-looking signals.
Cold chain temperature drift doesn't breach a threshold overnight. It approaches one over hours. A site dispensing faster than planned doesn't create a stockout in a day. It creates one over weeks. A CMO batch release delay doesn't derail a trial immediately. It initiates a cascade that takes six weeks to surface as patient impact.
Predictive detection requires pattern recognition across multiple data streams simultaneously; identifying the combination of signals that precede a problem. What we need is a system that identifies trajectory.
Without that predictive layer, we are always looking at the past. And in a Phase III trial with patients in chairs waiting for their infusion, the past is not where the problem gets solved.
What the Six-Week Gap Looks Like, Week by Week
| Week Number | What Happened | Why it wasn't caught |
|---|---|---|
| Week 16 | Three sites enrolling 15% above plan | Visible in CTMS but never reconciled against site inventory in WMS |
| Week 17 | Bridging batch at the CMO slips two weeks due to a raw material delay | SAP was updated but no connection was made to the sites now running above-plan enrollment |
| Week 18 | Depot replenishment order placed on standard lead-time assumptions | Enrollment acceleration had already consumed buffer stock faster than planned. No system flagged the gap. |
| Week 19 | Temperature telemetry logs a 45-minute excursion at one depot | Within MKT parameters, manually reviewed and closed. No connection made to the inventory risk building downstream. |
| Week 20 | Site coordinators begin requesting emergency shipments informally, drawing down depot stock further | Requests processed reactively. Weekly review deck circulated. Nobody connected enrollment, batch slip, and buffer depletion. |
| Week 21 | Depot inventory drops below safety stock threshold | Appeared in the weekly inventory report, reviewed on Monday morning |
| Week 22 | Monday, 6:47 AM. Warsaw. Patients in chairs. No drug. | The window to intervene closed six weeks ago |
Every single signal that could have prevented this by studying the data at Week 16. The real problem was the absence of a system capable of reading all of it simultaneously, in relationship to each other, and projecting what it meant for the trial six weeks ahead.
Where in the Clinical Trial Supply Chain Risk Actually Originates
Understanding why detection fails requires understanding where risk enters the clinical supply chain and how it travels.
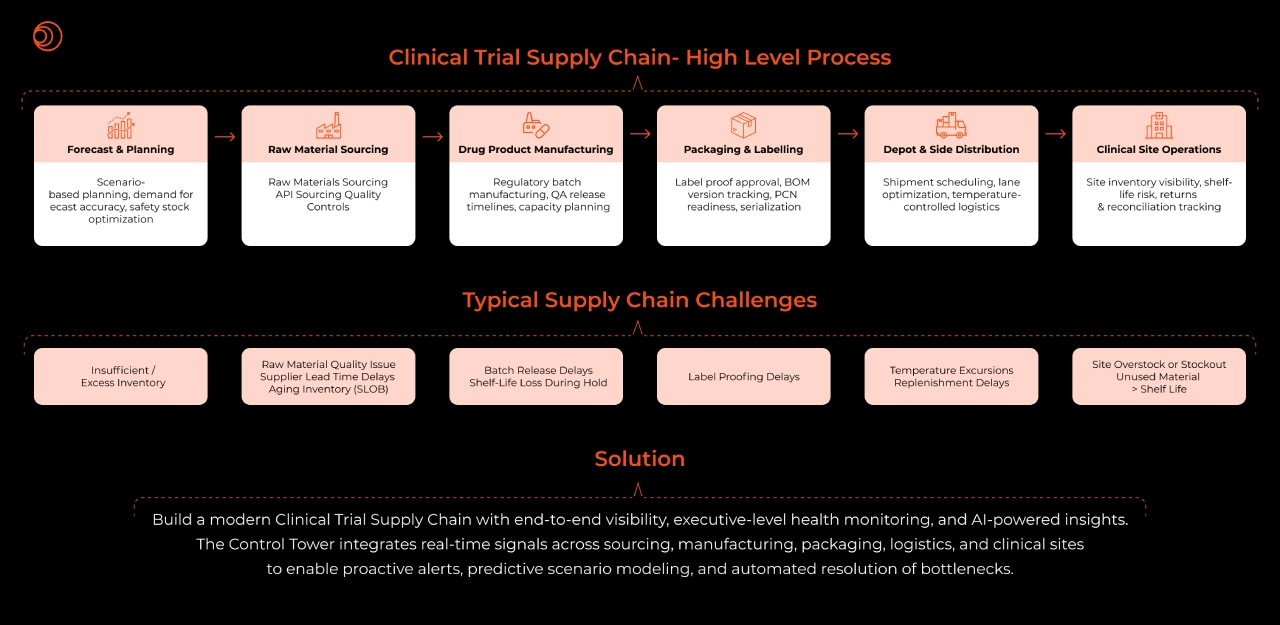
A clinical trial supply chain spans six interconnected stages, and each stage carries its own category of failure:
- Forecast and planning are where insufficient or excess inventory originates. Demand scenarios built on static assumptions do not flex when enrollment deviates, and enrollment almost always deviates.
- Raw material sourcing introduces supplier lead time delays, quality issues, and aging inventory. These are slow-moving risks that are rarely monitored with the frequency they require.
- Drug product manufacturing is where batch release delays and shelf-life loss during hold accumulate silently. A batch in regulatory review does not generate an alert when its release date slips past a critical replenishment window.
- Packaging and labelling introduce label proofing delays; one of the most underestimated sources of timeline risk in clinical operations.
- Depot and site distribution is where temperature excursions occur, and replenishment delays materialize. This is also where most organizations have the least real-time visibility.
- Clinical site operations are where everything upstream converges site overstock or stockout, unused material exceeding shelf life, and the patient who arrives for an infusion that isn't there.
The important observation is that by the time a risk becomes visible at the site level, it originated two or three stages earlier. A stockout at Site 14 in Warsaw was a raw material delay at the CMO, a batch release slip, and an enrollment acceleration that no one reconciled against available inventory — all of which happened weeks before the patient arrived.
Risk originates upstream and travels downstream, and every stage it crosses without detection makes it harder and more expensive to resolve.
What Closing the Gap Means in Clinical Trials Supply Chains
The question I am asked most frequently after walking through the six-week scenario is: what would have needed to be true for this to be caught in Week 16?
The answer is an architecture built around three capabilities that most clinical supply chain organizations do not currently have operating together.
Cross-system relationship mapping in real time
Integration in the sense of a continuous layer that maps live relationships between entities across systems; connecting a site's dispensing rate to its depot inventory to the planned batch release date and updates those relationships as new data flows in.
Trajectory detection, not threshold alerting
The clearest distinction between reactive and predictive supply chain intelligence is this: one tells you a threshold was breached, the other tells you a threshold will be breached unless something changes.
Cold chain monitoring is the clearest illustration. The average detection lag on a temperature excursion without predictive tooling is 48 to 72 hours. At that point the conversation shifts from prevention to damage control and whether a Fit-for-Use assessment can salvage the batch. A system that reads telemetry trajectories rather than point-in-time values can identify a developing excursion hours before it becomes a breach. That is the intervention window. That is where the damage is preventable.
The same logic applies to inventory. A site running 15% above enrollment plan is not a threshold breach on Day 1. It is a trajectory that, left unread in context, becomes a stockout six weeks later.
Decision support at the moment of the alert
When an alert fires 18 days before a projected stockout, the question is: emergency shipment, site reallocation, or enrollment adjustment — and what does each option cost in time, material, and patient access? A supply team equipped to answer that question in hours, not days, has genuinely closed the gap. A supply team that receives the alert and then spends two weeks in email chains has not.
The Business Case — Numbers I Stand Behind
I'm careful about the numbers I put in front of enterprise leaders, because I've seen too many AI ROI promises that don't survive contact with a CFO. These are numbers I've seen validated in real pharma deployments:
- 6 weeks → hours — reduction in the risk detection window with unified AI signal integration
- 20% reduction in site stockouts post AI platform go-live
- 60% improvement in write-off efficiency through predictive cold chain management and FFU decision support
- 600+ FTE hours per year recovered from manual investigation, report generation, and exception chasing
- $28M NPV across pharma deployments of the integrated platform
- 58% IRR on five-year AI platform investment
At $1.3 million per day of Phase III delay, a single avoided week of delay more than pays for a meaningful platform investment. But I always tell my clients: the number that matters most isn't on a spreadsheet. It's the patient who received their treatment on schedule. The biologic that reached the site in full integrity. The trial that completed without a protocol deviation on record.
The financial case makes the investment easy to approve. The patient impact is why it matters.
Read the full case study: Building an Intelligent Clinical Trial Control Tower
The Architectural Shift This Industry Needs
I have been in enough rooms where the conversation starts with "we need better dashboards" and ends with a vendor demo of more real-time data flowing into the same organizational processes that created the six-week gap in the first place.
But what pharma companies need is a mature clinical supply chain intelligence architecture that moves through layers: a unified data foundation that eliminates the silo problem, a control layer with KPI governance and audit, an intelligent layer capable of root cause analysis and scenario planning, an orchestration layer where autonomous workflows close loops without manual intervention, and a recommendation and experience layer where prescriptive guidance reaches the people who need it at the moment they need it.
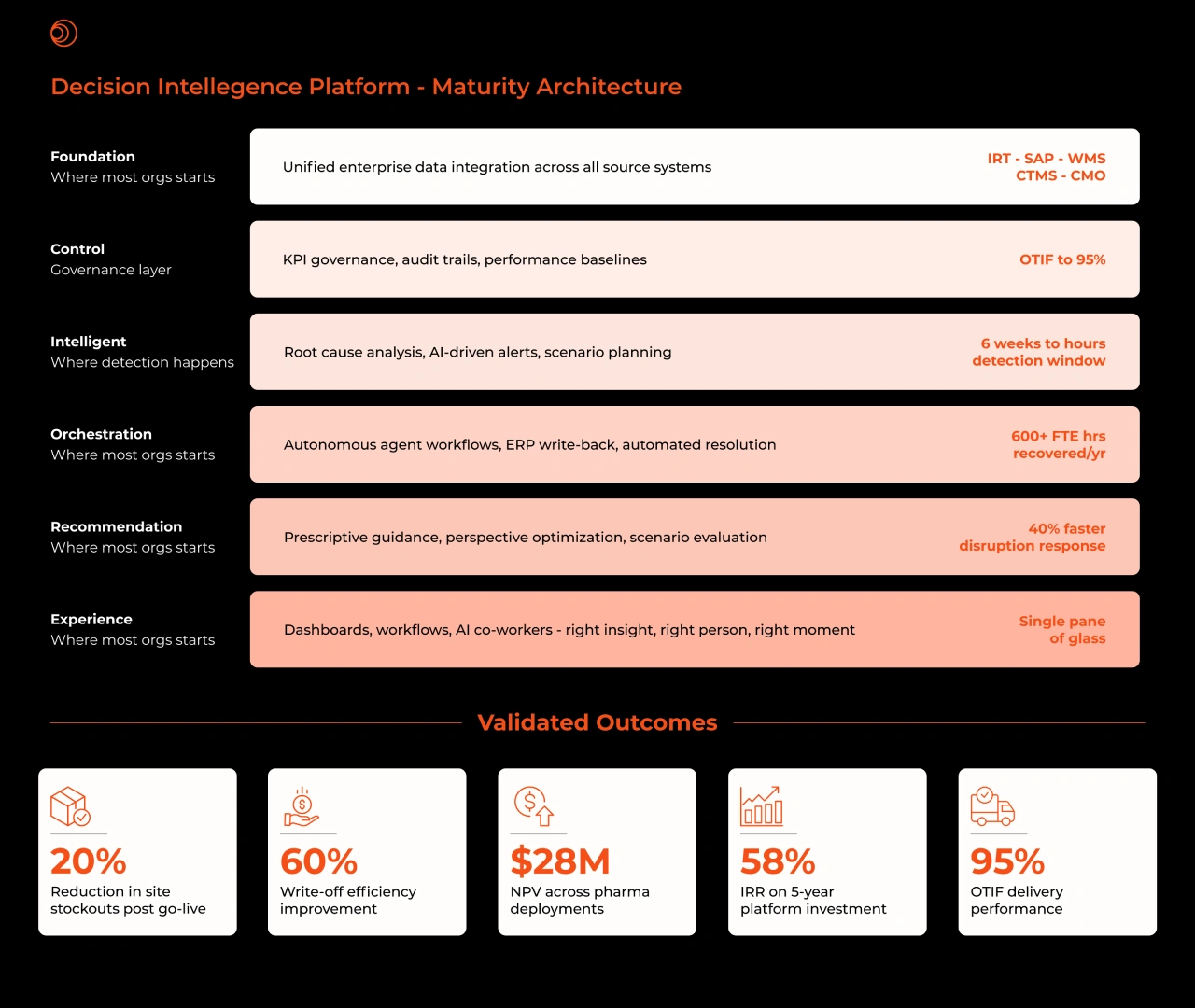
Most organizations are somewhere in the middle of this maturity curve. They have data. They have some integration. What they frequently lack is the intelligence and orchestration layers; the parts of the architecture that turn data into decisions rather than reports.
The data needed to have caught the Warsaw stockout at Week 16 existed. It existed in IRT, in SAP, in WMS, in CTMS, in the CMO portal. What did not exist was the layer that read it together, mapped the relationships, and projected the trajectory. That layer is buildable. The technology exists. The organizational commitment to prioritize it is what most clinical supply chains are still developing.
Explore how Syren's Clinical Trial Control Tower addresses the detection gap in clinical operations.